SURGICAL TREATMENT OF PECTUS CARINATUM (PIGEON CHEST) AND ABRAMSON PROCEDURE
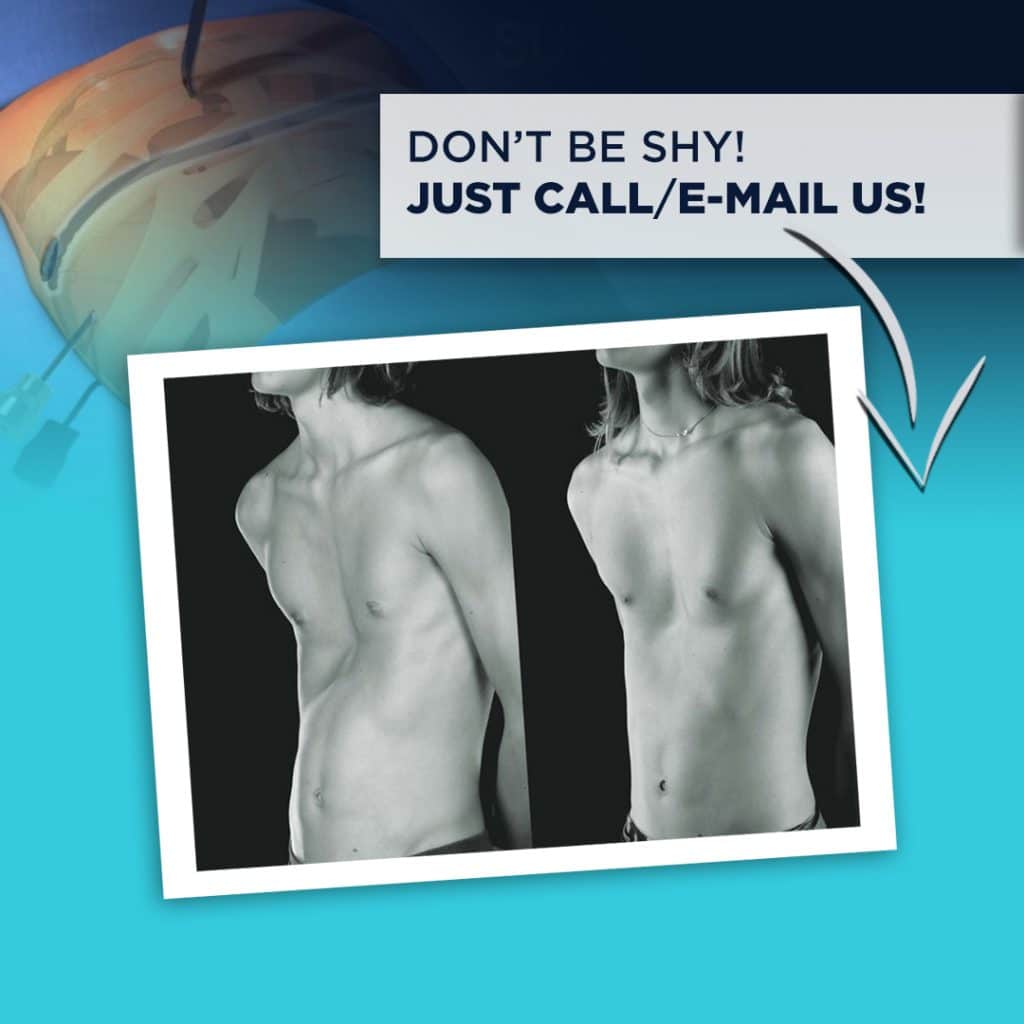
Image on the left is before Abramson procedure. Image on the right is after the procedure
Argentinian thoracic surgeon Dr. Horacio Abramson was the first to adapt the Nuss technique (minimally invasive technique to treat pectus carinatum patients) to treat pectus carinatum patients and share his findings in 2005 with the medical world (1).
After a five-year follow-up, he shared results acquired from 40 patients with the medical world. After the bar was removed the procedure was highly successful for 10, successful for 4, mediocre for 4, and unsuccessful for 2 out of 20 patients in total. The success rate of Abramson procedure is quite high as seen above. After the removal of the bar, results were positive for 18 out of 20 patients (2).
Before the Surgery;
- First, physical examination of the patient is conducted.
- The patient and patient’s relative is informed thoroughly and their questions are answered, in order for them to be able to make an informed decision about the pectus carinatum treatment.
- To determine the level of chest deformation a two sided chest graphy (front and side-back) and tomography of the chest is taken. According to Haller index, if the proportion of horizontal length of the chest to its vertical length is greater than 2.5 the case is taken into serious consideration. If the proportion is greater than 3.5 the patient may consider surgical treatment.
- Blood tests and respiratory function tests are conducted to determine whether the patient is fit for general anesthesia.
- Cardiology consultation is necessary to determine whether the patient has a heart condition. If necessary EKG and EKO tests are conducted to find a possible heart condition, if the patient indeed has a heart condition, it should be treated first in order to proceed with pectus excavatum treatment.
- For those patients with internal diseases specific consultations are necessary.
- The patient and patient’s relative re informed about alternative treatment methods and success rates.
- Patient’s questions about her condition and the procedure are answered prior to te operation.
Success rates of open surgery and Abramson procedure which is an endoscopic minimally invasive procedure are similar. However, Abramson procedure have become widespread due to lower chance of complications during and after the surgery, early discharge and quicker adaptation to daily life (2 weeks).
The preferred ages for the operation is 7 – 14. Between these ages bone structure of the thoracic wall is softer making the procedure less challenging. Also following the procedure thoracic wall can grow into its natural anatomical position. These being said, success rate is similar for adults (3).
Abramson Procedure
Abramson procedure is conducted under general anesthesia and it takes around 60 minutes. First, from the right side of the thoracic wall, close to the underarm a 2 centimeter incision is made to reach the thoracic wall.
Lorenz Pectus Bar – Erkan Yıldırım, MD.
A tunnel is opened by PVC (polyvinyl chloride) tube and trocar from one side of the thoracic wall to the other through the incision. This tunnel passes from the front of the sternum (where it bulges the most) under the pectoral muscles.
On the other side of the thoracic wall another 2 centimeter incision is made to open an exit for the tunnel.
A steel bar (Lorenz Pectus) is implanted to push down the bulge on the chest.
Attaching the Stabilizer to the Bones
Lorenz Bar (Pectus Bar) is chosen according to the chest size and shape of the patient and the two ends of the bar are given the necessary curve before the operation. Pectus Bar is introduced into the tunnel from one end and it is pushed through until it reaches the other end of the tunnel. Once it does, the bar has reached its final position.
When the bar reaches the other side of the thoracic wall, the PVC tube is removed. Before or after the bar is inserted into the tunnel, stabilizers are placed onto the ribs with steel stitches.
Once the sternum is in the desired position, incisions are stitched up and the procedure concluded. You can get detailed information on Abramson Procedure in medical publications (4).
Removing the Bars
Depending on the patient’s age and the state of the sternum, the bar is removed within 2 – 4 years with a 30 minute procedure under general anesthesia.
Risks of the Procedure
Generally risks of the operation is very low (5). Pneumothorax (1 out of 40 patients – air leaking into the space between the chest wall and the lung), infection of wounds (1 out of 40 patients), inflammation in the scars (6 out of 40 patients), coming off of steel stitches (3 out of 40 patients). Infecting scars occurs less than 0.7% of patients (6).
Reference
- Arch Bronconeumol. 2005;41(6):349-51 and J Pediatr Surg. 2009;44(1):118-24.
- Pediatr Surg. 2009;44(1):118–24.
- http://icvts.ctsnetjournals.org/cgi/content/full/9/suppl_1/S1.
- Arch Bronconeumol. 2005; 41:349-51 ve Journal of Pediatric Surgery, 44 (1), Jan 2009, p. 118-124.
- Pediatr Surg. 2009;44(1):118-24).
- http://icvts.ctsnetjournals.org/cgi/content/full/9/suppl_1/S1.